Massachusetts Alliance of Juvenile Court Clinics
(Line Item 5055-0000)
Every year, thousands of the Commonwealth’s most vulnerable, under-resourced children and families appear before the Massachusetts Juvenile Courts. Over 70% face a combination of mental health and behavioral problems, medical issues, substance use, histories of abuse and neglect, learning disabilities, and acculturation stressors. The Juvenile Court Clinics assist the Court with the most complicated cases.
The Juvenile Court Clinics were established with the statewide Juvenile Court in 1993. The Juvenile Court continues to respond to changes brought about by the COVID-19 pandemic and Criminal Justice Reform Legislation passed in 2018, which changed the age of Juvenile Court jurisdiction on delinquency matters to age 12 to 18 (previously age 7 to 18) and expanded Diversion and Restorative Justice programs.
We want to thank the Legislature for sustaining the FY23 increase of $1.5 Million in FY24. Maintaining these funds in FY24 helped to support the retention and recruitment of highly-specialized clinical staff; however, the Juvenile Court Clinics continue to struggle to retain and recruit clinical staff.
Now, in FY25 we ask that the Legislature increase funding by $1.5 Million beyond the FY24 level of support. Staffing challenges persist, prompting the need for salary increases for employee retention, advance-ment, and recruitment. Many years of inadequate funding have resulted in a system-wide struggle to simply catch up. Increased funding in FY25 is essential to sustain the meaningful gains made with the FY23 and FY24 appropriations. Increased funding will support retention, recruitment and expansion of forensic staff required to meet the clinical needs of under-resourced, court-involved children and families:
- Children and families continuing to experience the lingering impacts of COVID-19.
- Children suffering from trauma due to parental/caregiver neglect and abuse, violence in their schools/communities, and/or are at-risk for sexual exploitation.
- Children with substance use problems requiring emergency out-of-home care through a court order, or specialized help to access limited community-based outpatient services.
- Children with Child Requiring Assistance matters who have not improved despite intensive, comprehensive home-based services, and are at risk for out-of-home placement.
- Children with Autism Spectrum Disorder requiring specialized assessment to understand behaviors that could impact their involvement with the juvenile justice system.
- Children who are Dual-Status Youth, involvedin both the child welfare and the juvenile justice systems, and at-risk for further involvement with the juvenile justice system.
- Children with multiple, complex issues who fall between the cracks of state agencies such as DCF, DMH, DYS, DDS and DPH and challenge the resources of the Family Resource Centers (FRCs) and the newly developed Community Behavioral Health Centers (CBHCs).
- Parents who require advocacy and guidance to access services specific to their family’s unique needs.
- Children who are older, since the Juvenile Court has jurisdiction over children up to age 18.
- Children who fail to meet criteria for Competence to Stand Trial and require repeated evaluations.
- Children boarding for days or weeks in hospital emergency rooms awaiting in-patient care.
- Parents before the Juvenile Court due to neglect and abuse of their children.
The Role of the Juvenile Court Clinics
Psychologists, social workers, and other mental health professionals at the Juvenile Court Clinics provide court-ordered evaluations, interventions, and referral services. All clinicians must be specially trained and credentialed by DMH. The Juvenile Court Clinics assist the Court in balancing the interests among child and family-centered interventions, public safety, and protection of children from abuse and neglect, while providing the following:
- Emergency evaluations of youth in crisis—for example, an evaluation of a 15-year-old boy who threatened to kill himself while at Court, or a Section 35 evaluation of a 17-year-old girl brought in for an emergency substance use evaluation because of her opioid abuse while on the run.
- Comprehensive psychosocial evaluations—such as evaluating a 14-year-old boy with an extensive trauma history who injured another youth. During the evaluation, the clinician also works with the family, school, and child-serving agencies in the community to seek appropriate treatment and service planning.
- Case management services—such as helping the Spanish-speaking family of a 13-year-old boy with chronic truancy navigate waitlists and other barriers to services, such as language capacity, transportation, and housing.
- Participation in diversionary, community-based initiatives—for example, in the Juvenile Detention Alternatives Initiative (JDAI), Dual-Status Youth (DSY) Programs, and System of Care (SOC) meetings.
- Evaluations to assess Competency to Stand Trial—for example, an evaluation of whether a 12-year-old boy, charged with assault and battery after he injured a classmate in a fight at school, could assist his lawyer in participating in his defense. The need for competency evaluations is rising as more youth come before the Juvenile Court with mental health issues, cognitive limitations and special needs, as well as immaturity.
- Specialized risk assessments and evaluations of substance use, sexual offending, aggressive behavior and fire setting—behavior typically related to a range of complex underlying problems. All evaluations include recommendations for appropriate treatment.
- Specialized evaluations in Care and Protection cases. These include evaluations of parenting capacity, evaluations of mental health concerns, and competency of a parent to assist their lawyer in court proceedings.
- Consultation to the Court and the community—Consultation to families, schools, community providers, state agencies, and others, regarding how the complex and rapidly changing service delivery systems may prevent a child’s further court involvement or the need for more intrusive and extensive interventions.
Cost Benefits of Juvenile Court Clinics
- Research indicates that saving one high-risk youth from heavy drug use, dropping out of school, and a life of crime saves society an average of $5 Million. Providing the Juvenile Court with recommendations for structured, community-based treatment and services that maintain public safety can prevent unnecessary detention, which has been estimated to cost the Commonwealth $120,000 annually per juvenile.
- Mental illnesses are serious medical illnesses that fall along a continuum of severity. Without treatment, the consequences of mental illness for the individual and society are staggering—unnecessary disability, unemployment, substance use, homelessness, inappropriate incarceration, suicide, and wasted lives—costing $100 Billion each year in the United States, according to the National Alliance on Mental Illness.
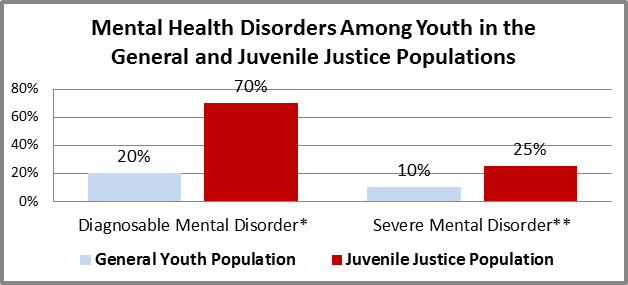
*An individual exhibiting behavioral or psychological symptoms that impact multiple life areas or create distress.
**A mental disorder so severe that an individual’s ability to perform routine daily tasks is significantly impaired.
